

How To Repair Small Left Inguinal Hernia Containing Fat
| Inguinal hernia | |
|---|---|
 | |
| Diagram of an indirect, scrotal inguinal hernia (median view from the left). | |
| Pronunciation | |
| Specialty | Full general surgery |
| Symptoms | Pain, bulging in the groin[1] |
| Complications | Strangulation[1] |
| Usual onset | < 1 year sometime, > 50 years quondam[2] |
| Gamble factors | Family history, smoking, chronic obstructive pulmonary disease, obesity, pregnancy, peritoneal dialysis, collagen vascular disease, connective tissue illness, previous open appendectomy[ane] [2] [three] |
| Diagnostic method | Based on symptoms, medical imaging[1] |
| Treatment | Bourgeois, surgery[1] |
| Frequency | 27% (males), 3% (females)[1] |
| Deaths | 59,800 (2015)[4] |
An inguinal hernia is a hernia (protrusion) of abdominal-cavity contents through the inguinal culvert. Symptoms are absent in near a tertiary of patients. This may include pain or discomfort especially with or following coughing, exercise, or bowel movements. Oftentimes it gets worse throughout the mean solar day and improves when lying down. A bulging area may occur that becomes larger when begetting down. Inguinal hernias occur more often on the correct than left side. The principal business organisation is strangulation, where the claret supply to part of the intestine is blocked. This usually produces severe hurting and tenderness of the area.[1]
Take chances factors for the evolution of a hernia include: smoking, chronic obstructive pulmonary disease, obesity, pregnancy, peritoneal dialysis, collagen vascular affliction, and previous open up appendectomy, amidst others.[1] [2] Predisposition to hernias is genetic[5] and they occur more than often in certain families.[6] [7] [viii] [one] Deleterious mutations causing predisposition to hernias seem to have dominant inheritance (specially for men). It is unclear if inguinal hernias are associated with heavy lifting. Hernias tin can often be diagnosed based on signs and symptoms. Occasionally medical imaging is used to confirm the diagnosis or rule out other possible causes.[1]
Groin hernias that do non crusade symptoms in males do not demand to be repaired. Repair, notwithstanding, is generally recommended in females due to the college rate of femoral hernias which have more complications. If strangulation occurs immediate surgery is required. Repair may be done by open up surgery or past laparoscopic surgery. Open surgery has the do good of possibly beingness done under local anesthesia rather than general anesthesia. Laparoscopic surgery mostly has less pain following the process.[1] [ix]
In 2022 inguinal, femoral and abdominal hernias affected near 18.5 million people.[10] About 27% of males and 3% of females develop a groin hernia at some time in their life.[1] Groin hernias occur most often before the historic period of one and after the historic period of 50.[2] Globally, inguinal, femoral and abdominal hernias resulted in threescore,000 deaths in 2022 and 55,000 in 1990.[4] [11]
Signs and symptoms [edit]

Frontal view of an inguinal hernia (correct).
Hernias usually present as bulges in the groin area that can go more prominent when coughing, straining, or standing upwardly. The bulge normally disappears on lying down. Mild discomfort can develop over time. The disability to "reduce", or place the burl back into the abdomen unremarkably means the hernia is 'incarcerated' which requires emergency surgery.
Every bit the hernia progresses, contents of the abdominal cavity, such as the intestines, can descend into the hernia and run the risk of being pinched inside the hernia, causing an intestinal obstacle. Significant pain at the hernia site is suggestive of a more severe course, such every bit incarceration (the hernia cannot be reduced back into the abdomen) and subsequent ischemia and strangulation (when the hernia becomes deprived of blood supply).[12] If the blood supply of the portion of the intestine caught in the hernia is compromised, the hernia is deemed "strangulated" and gut ischemia and gangrene can issue, with potentially fatal consequences. The timing of complications is non predictable.
Pathophysiology [edit]
In males, indirect hernias follow the same route as the descending testes, which migrate from the abdomen into the scrotum during the development of the urinary and reproductive organs. The larger size of their inguinal canal, which transmitted the testicle and accommodates the structures of the spermatic cord, might be one reason why men are 25 times more than likely to accept an inguinal hernia than women. Although several mechanisms such as strength of the posterior wall of the inguinal culvert and shutter mechanisms compensating for raised intra-abdominal pressure prevent hernia germination in normal individuals, the exact importance of each gene is still under debate. The physiological schoolhouse of thought thinks that the take chances of hernia is due to a physiological departure between patients who suffer hernia and those who do not, namely the presence of aponeurotic extensions from the transversus abdominis aponeurotic arch.[xiii]
Inguinal hernias more often than not contain the omentum or a part of the small intestines, however, some unusual contents may be an appendicitis, diverticulitis, colon cancer, urinary bladder, ovaries, and rarely cancerous lesions.[14]
-

Illustration of an inguinal hernia.
-

Different types of inguinal hernias.
-

Inguinal fossae
Diagnosis [edit]

An incarcerated inguinal hernia as seen on cross exclusive CT scan

A frontal view of an incarcerated inguinal hernia (on the patient's left side) with dilated loops of bowel above.

An inguinal hernia which contains part of the bladder. Bladder cancer besides present.
There are two types of inguinal hernia, direct and indirect, which are defined past their human relationship to the junior epigastric vessels. Direct inguinal hernias occur medial to the inferior epigastric vessels when abdominal contents herniate through a weak spot in the fascia of the posterior wall of the inguinal canal, which is formed past the transversalis fascia. Indirect inguinal hernias occur when abdominal contents protrude through the deep inguinal ring, lateral to the junior epigastric vessels; this may be caused by failure of embryonic closure of the processus vaginalis.
In the case of the female, the opening of the superficial inguinal ring is smaller than that of the male. As a outcome, the possibility for hernias through the inguinal canal in males is much greater because they accept a larger opening and therefore a much weaker wall through which the intestines may protrude.
| Type | Clarification | Human relationship to inferior epigastric vessels | Covered past internal spermatic fascia? | Usual onset |
|---|---|---|---|---|
| indirect inguinal hernia | protrudes through the inguinal band and is ultimately the result of the failure of embryonic closure of the processus vaginalis after the testicle passes through information technology | Lateral | Yes | Congenital / Adult |
| directly inguinal hernia | enters through a weak point in the fascia of the intestinal wall (Hesselbach triangle) | Medial | No | Developed |
Inguinal hernias, in turn, belong to groin hernias, which also includes femoral hernias. A femoral hernia is not via the inguinal canal, but via the femoral canal, which normally allows passage of the common femoral artery and vein from the pelvis to the leg.
In Amyand's hernia, the content of the hernial sac is the vermiform appendix.
Ultrasound paradigm of inguinal hernia. Moving intestines in inguinal canal with respiration.
In Littre's hernia, the content of the hernial sac contains a Meckel's diverticulum.
Clinical classification of hernia is also important according to which hernia is classified into
- Reducible hernia: is one which tin can be pushed back into the abdomen by putting manual pressure to it.
- Irreducible/Incarcerated hernia: is 1 which cannot be pushed dorsum into the abdomen by applying manual pressure.
Irreducible hernias are farther classified into
- Obstructed hernia: is one in which the lumen of the herniated part of intestine is obstructed.
- Strangulated hernia: is one in which the claret supply of the hernia contents is cut off, thus, leading to ischemia. The lumen of the intestine may exist patent or not.
Direct inguinal hernia [edit]
The direct inguinal hernia enters through a weak point in the fascia of the abdominal wall, and its sac is noted to be medial to the inferior epigastric vessels. Straight inguinal hernias may occur in males or females, merely males are ten times more likely to become a direct inguinal hernia.[15]
A direct inguinal hernia protrudes through a weakened area in the transversalis fascia about the medial inguinal fossa inside an anatomic region known as the inguinal or Hesselbach'southward triangle, an area defined past the edge of the rectus abdominis muscle, the inguinal ligament and the inferior epigastric artery. These hernias are capable of exiting via the superficial inguinal ring and are unable to extend into the scrotum.
When a patient suffers a simultaneous direct and indirect hernia on the same side, it is called a pantaloon hernia or saddlebag hernia because it resembles a pair of pants with the epigastric vessels in the crotch, and the defects can be repaired separately or together. Another term for pantaloon hernia is Romberg's hernia.
Since the abdominal walls weaken with historic period, direct hernias tend to occur in the middle-aged and elderly. This is in dissimilarity to indirect hernias which tin occur at any age including the young, since their etiology includes a congenital component where the inguinal canal is left more than patent (compared to individuals less susceptible to indirect hernias).[16] [17] Additional risk factors include chronic constipation, overweight/obesity, chronic cough, family history and prior episodes of direct inguinal hernias.[15]
Indirect inguinal hernia [edit]

Ultrasound of an indirect hernia containing fat, with testicle seen at correct.
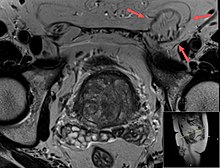
T2 weighted MRI of the aforementioned instance (done for another purpose), also demonstrating fat content.
Ultrasound showing an indirect inguinal hernia[18]
Incarcerated inguinal hernia[19]
An indirect inguinal hernia results from the failure of embryonic closure of the deep inguinal band after the testicle has passed through it. Information technology is the almost common cause of groin hernia. A double indirect inguinal hernia has two sacs.
In the male fetus, the peritoneum gives a coat to the testicle every bit it passes through this ring, forming a temporary connection chosen the processus vaginalis. In normal development, the processus is obliterated in one case the testicle is completely descended. The permanent coat of peritoneum that remains around the testicle is called the tunica vaginalis. The testicle remains continued to its claret vessels and the vas deferens, which make up the spermatic cord and descend through the inguinal canal to the scrotum.
The deep inguinal band, which is the showtime of the inguinal canal, remains every bit an opening in the fascia transversalis, which forms the fascial inner wall of the spermatic cord. When the opening is larger than necessary for passage of the spermatic cord, the stage is set for an indirect inguinal hernia. The protrusion of peritoneum through the internal inguinal ring tin exist considered an incomplete obliteration of the processus.
In an indirect inguinal hernia, the protrusion passes through the deep inguinal ring and is located lateral to the inferior epigastric artery. Hence, the conjoint tendon is non weakened.
There are 3 master types
- Bubonocele: in this instance the hernia is limited in inguinal canal.
- Funicular: here the processus vaginalis is closed at its lower finish only above the epididymis. The content of the hernial sac can be felt separately from the testis which lies below the hernia.
- Complete (or scrotal): here the processus vaginalis is patent throughout. The hernial sac is continuous with the tunica vaginalis of the testis. The hernia descends downwards to the bottom of the scrotum and it is difficult to differentiate the testis from hernia.
In the female person, groin hernias are simply 4% as common as in males. Indirect inguinal hernia is nonetheless the most common groin hernia for females. If a woman has an indirect inguinal hernia, her internal inguinal ring is patent, which is aberrant for females. The protrusion of peritoneum is not chosen "processus vaginalis" in women, as this structure is related to the migration of the testicle to the scrotum. It is but a hernia sac. The eventual destination of the hernia contents for a adult female is the labium majus on the aforementioned side, and hernias can enlarge one labium dramatically if they are immune to progress.
Medical imaging [edit]
A physician may diagnose an inguinal hernia, as well every bit the type, from medical history and physical exam.[20] For confirmation or in uncertain cases, medical ultrasonography is the first pick of imaging, because it tin can both discover the hernia and evaluate its changes with for instance pressure, continuing and Valsalva maneuver.[21]
When assessed by ultrasound or cross exclusive imaging with CT or MRI, the major differential in diagnosing indirect inguinal hernias is differentiation from spermatic cord lipomas, every bit both can incorporate just fat and extend forth the inguinal canal into the scrotum.[22]
On axial CT, lipomas originate inferior or lateral to the string, and are located inside the cremaster muscle, while inguinal hernias prevarication anteromedial to the cord and are not intramuscular. Large lipomas may appear nearly indistinguishable equally the fatty engulfs anatomic boundaries, but they do not alter position with coughing or straining.[22]
Differential diagnosis [edit]
Differential diagnosis of the symptoms of inguinal hernia mainly includes the post-obit potential weather:[23]
- Femoral hernia
- Epididymitis
- Testicular torsion
- Lipomas
- Inguinal adenopathy (Lymph node Swelling)
- Groin abscess
- Saphenous vein dilation, called Saphena varix
- Vascular aneurysm or pseudoaneurysm
- Hydrocele
- Varicocele
- Cryptorchidism (Undescended testes)
Management [edit]
Conservative [edit]
There is currently no medical recommendation almost how to manage an inguinal hernia status in adults, due to the fact that, until recently,[24] [25] elective surgery used to be recommended. The hernia truss (or hernia chugalug) is intended to contain a reducible inguinal hernia inside the belly. Information technology is not considered to provide a cure, and if the pads are hard and intrude into the hernia aperture they may cause scarring and enlargement of the aperture. In addition, most trusses with older designs are non able effectively to contain the hernia at all times, because their pads exercise not remain permanently in contact with the hernia. The more mod multifariousness of truss is made with non-intrusive flat pads and comes with a guarantee to concur the hernia securely during all activities. They have been described past users as providing greater confidence and comfort when carrying out physically demanding tasks.[ citation needed ] Notwithstanding, their utilize is controversial, as information to decide whether they help prevent hernia complications are lacking.[i] A truss also increases the probability of complications, which include strangulation of the hernia, cloudburst of the spermatic cord, and atrophy of the fascial margins. This allows the defect to enlarge and makes subsequent repair more difficult.[26] Their popularity is notwithstanding likely to increase, as many individuals with small, painless hernias are at present delaying hernia surgery due to the run a risk of post-herniorrhaphy hurting syndrome.[27] Elasticated pants used by athletes may too provide useful support for the smaller hernia.[ citation needed ]
Surgical [edit]

Surgical incision in groin subsequently inguinal hernia operation
Surgical correction of inguinal hernias is chosen a hernia repair. It is non recommended in minimally symptomatic hernias, for which watchful waiting is advised, due to the risk of post herniorraphy hurting syndrome. Surgery is commonly performed as outpatient surgery. At that place are various surgical strategies which may be considered in the planning of inguinal hernia repair. These include the consideration of mesh apply (e.thousand. synthetic or biologic), open repair, apply of laparoscopy, type of anesthesia (full general or local), appropriateness of bilateral repair, etc. Mesh or non mesh repairs have both benefits in different areas, merely mesh repairs may reduce the rate of hernia reappearance, visceral or neurovascular injuries, length of hospital stay and time to return to activities of daily living. [28] Laparoscopy is almost ordinarily used for non-emergency cases; notwithstanding, a minimally invasive open up repair may have a lower incidence of mail-operative nausea and mesh associated pain. During surgery conducted under local anaesthesia, the patient volition be asked to cough and strain during the procedure to help in demonstrating that the repair is without tension and sound.[29]
Constipation after hernia repair results in strain to evacuate the bowel causing pain, and fearfulness that the sutures may rupture. Opioid analgesia makes constipation worse. Promoting an easy bowel motion is important mail-operatively.
Surgical correction is e'er recommended for inguinal hernias in children.[30]
Emergency surgery for incarceration and strangulation acquit much higher risk than planned, "constituent" procedures. Notwithstanding, the risk of incarceration is depression, evaluated at 0.ii% per twelvemonth.[31] On the other hand, surgery has a risk of inguinodynia (10-12%), and this is why males with minimal symptoms are advised to watchful waiting.[31] [32] Still, if they experience discomfort while doing physical activities or they routinely avoid them for fear of pain, they should seek surgical evaluation.[33] For female patients, surgery is recommended even for asymptomatic patients.[34]
Epidemiology [edit]
A direct inguinal hernia is less common (~25–30% of inguinal hernias) and usually occurs in men over twoscore years of historic period.
Men have an viii times higher incidence of inguinal hernia than women.[35]
Meet also [edit]
- Birkett hernia
References [edit]
- ^ a b c d e f one thousand h i j 1000 l 1000 Fitzgibbons RJ, Jr; Forse, RA (xix February 2022). "Clinical practice. Groin hernias in adults" (PDF). The New England Journal of Medicine. 372 (8): 756–63. doi:ten.1056/NEJMcp1404068. PMID 25693015.
- ^ a b c d Domino, Frank J. (2014). The 5-infinitesimal clinical consult 2022 (22nd ed.). Philadelphia, Pa.: Wolters Kluwer Wellness/Lippincott Williams & Wilkins. p. 562. ISBN9781451188509.
- ^ Burcharth J, Pommergaard HC, Rosenberg J (2013). "The inheritance of groin hernia: a systematic review". Hernia. 17 (two): 183–9. doi:ten.1007/s10029-013-1060-four. PMID 23423330. S2CID 27799467.
- ^ a b GBD 2022 Mortality and Causes of Death, Collaborators. (8 Oct 2022). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2022". Lancet. 388 (10053): 1459–1544. doi:10.1016/S0140-6736(xvi)31012-i. PMC5388903. PMID 27733281.
- ^ Öberg, S.; Andresen, K.; Rosenberg, J. (2017). "Etiology of Inguinal Hernias: A Comprehensive Review". Frontiers in Surgery. 4: 52. doi:ten.3389/fsurg.2017.00052. PMC5614933. PMID 29018803.
- ^ Mihailov, E.; Nikopensius, T.; Reigo, A.; Nikkolo, C.; Kals, M.; Aruaas, Grand.; Milani, 50.; Seepter, H.; Metspalu, A. (2017). "Whole-exome Sequencing Identifies a Potential TTN Mutation in a Multiplex Family With Inguinal Hernia - PubMed". Hernia : The Journal of Hernias and Abdominal Wall Surgery. 21 (1): 95–100. doi:10.1007/s10029-016-1491-ix. PMC5281683. PMID 27115767.
- ^ Sezer, Southward.; Şimşek, Northward.; Celik, H. T.; Erden, Thousand.; Ozturk, Yard.; Düzgün, A. P.; Çoşkun, F.; Demircan, 1000. (2014). "Association of Collagen Blazon I Blastoff ane Factor Polymorphism With Inguinal Hernia - PubMed". Hernia : The Journal of Hernias and Abdominal Wall Surgery. 18 (four): 507–12. doi:10.1007/s10029-013-1147-y. PMID 23925543. S2CID 22999363.
- ^ Gong, Y.; Shao, C.; Sun, Q.; Chen, B.; Jiang, Y.; Guo, C.; Wei, J.; Guo, Y. (1994). "Genetic Study of Indirect Inguinal Hernia - PubMed". Journal of Medical Genetics. 31 (iii): 187–92. doi:10.1136/jmg.31.3.187. PMC1049739. PMID 8014965.
- ^ Simons MP, Aufenacker T, Bay-Nielsen 1000, et al. (August 2009). "European Hernia Order guidelines on the treatment of inguinal hernia in adult patients". Hernia. 13 (4): 343–403. doi:x.1007/s10029-009-0529-7. PMC2719730. PMID 19636493.
- ^ GBD 2022 Disease and Injury Incidence and Prevalence, Collaborators. (8 Oct 2022). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Report 2022". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(sixteen)31678-6. PMC5055577. PMID 27733282.
- ^ GBD 2022 Mortality and Causes of Death, Collaborators (17 December 2022). "Global, regional, and national age-sexual practice specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2022". Lancet. 385 (9963): 117–71. doi:10.1016/S0140-6736(fourteen)61682-2. PMC4340604. PMID 25530442.
- ^ Neutra, Raymond; Velez, Adolfo; Ferrada, Ricardo; Galan, Ricardo (January 1981). "Risk of incarceration of inguinal hernia in Cali, Colombia". Periodical of Chronic Diseases. 34 (11): 561–564. doi:10.1016/0021-9681(81)90018-7. PMID 7287860.
- ^ Desarda, Mohan P (16 April 2003). "Surgical physiology of inguinal hernia repair - a written report of 200 cases". BMC Surgery. three (1): 2. doi:x.1186/1471-2482-3-2. PMC155644. PMID 12697071.
- ^ Yoell, John H. (September 1959). "SURPRISES IN HERNIAL SACS—Diagnosis of Tumors by Microscopic Exam". California Medicine. 91 (three): 146–148. ISSN 0008-1264. PMC1577810. PMID 13846556.
- ^ a b "Direct Inguinal Hernia". University of Connecticut. Archived from the original on April 27, 2022. Retrieved May 6, 2022.
- ^ James Harmon M.D. Lecture 13. Human Gross Anatomy. University of Minnesota. September 4, 2008.
- ^ http://www.emedicinehealth.com/hernia/article_em.htm
- ^ "UOTW #16 - Ultrasound of the Week". Ultrasound of the Calendar week. 2 September 2022. Retrieved 27 May 2022.
- ^ "UOTW #40 - Ultrasound of the Week". Ultrasound of the Week. 9 March 2022.
- ^ LeBlanc, Kim Edward; LeBlanc, Leanne L; LeBlanc, Karl A (15 June 2022). "Inguinal hernias: diagnosis and management". American Family Physician. 87 (12): 844–8. PMID 23939566.
- ^ Stavros, A. Thomas; Rapp, Cindy (September 2022). "Dynamic Ultrasound of Hernias of the Groin and Inductive Intestinal Wall". Ultrasound Quarterly. 26 (three): 135–169. doi:10.1097/RUQ.0b013e3181f0b23f. PMID 20823750. S2CID 31835133.
- ^ a b Burkhardt, Joan Hu; Arshanskiy, Yevgeniy; Munson, J. Lawrence; Scholz, Francis J. (March 2022). "Diagnosis of Inguinal Region Hernias with Axial CT: The Lateral Crescent Sign and Other Key Findings". RadioGraphics. 31 (ii): E1–E12. doi:ten.1148/rg.312105129. PMID 21415178.
- ^ Klingensmith ME, Chen LE, Glasgow SC, Goers TA, Melby SJ (2008). The Washington manual of surgery. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN978-0-7817-7447-5.
- ^ Simons MP, Aufenacker T, Bay-Nielsen Yard, Bouillot JL, Campanelli Thou, Conze J, et al. (August 2009). "European Hernia Guild guidelines on the treatment of inguinal hernia in adult patients". Hernia. 13 (4): 343–403. doi:10.1007/s10029-009-0529-7. PMC2719730. PMID 19636493.
- ^ Rosenberg J, Bisgaard T, Kehlet H, Wara P, Asmussen T, Juul P, Strand L, Andersen FH, Bay-Nielsen M (February 2022). "Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults". Dan Med Balderdash. 58 (2): C4243. PMID 21299930.
- ^ Purkayastha S, Chow A, Athanasiou T, Tekkis P, Darzi A (July 2008). "Inguinal hernia". BMJ Clin Evid. 2008. PMC2908002. PMID 19445744.
- ^ Aasvang Due east, Kehlet H (July 2005). "Chronic postoperative pain: the instance of inguinal herniorrhaphy". Br J Anaesth. 95 (1): 69–76. doi:10.1093/bja/aei019. PMID 15531621.
- ^ Lockhart, Kathleen; Dunn, Douglas; Teo, Shawn; Ng, Jessica Y.; Dhillon, Manvinder; Teo, Edward; Van Driel, Mieke L. (2018). "Mesh versus non‐mesh for inguinal and femoral hernia repair". Cochrane Database of Systematic Reviews. 2018 (9): CD011517. doi:10.1002/14651858.CD011517.pub2. PMC6513260. PMID 30209805.
- ^ Inguinal Hernia Archived 2007-09-27 at the Wayback Machine
- ^ "Inguinal Hernia". UCSF Pediatric Surgery.
- ^ a b Fitzgibbons, Robert J.; Giobbie-Hurder, Anita; Gibbs, James O.; Dunlop, Dorothy D.; Reda, Domenic J.; McCarthy, Martin; Neumayer, Leigh A.; Barkun, Jeffrey S. T.; Hoehn, James L.; Murphy, Joseph T.; Sarosi, George A.; Syme, William C.; Thompson, Jon S.; Wang, Jia; Jonasson, Olga (xviii January 2006). "Watchful Waiting vs Repair of Inguinal Hernia in Minimally Symptomatic Men". JAMA. 295 (3): 285–92. doi:10.1001/jama.295.3.285. PMID 16418463.
- ^ Simons, MP; Aufenacker, TJ; Berrevoet, F; Bingener, J; Bisgaard, T; Bittner, R; Bonjer, HJ; Coffin, M; Campanelli, G (2017). World guidelines for groin hernia management (PDF).
- ^ Brooks, David. "Overview of treatment for inguinal and femoral hernia in adults". www.uptodate.com . Retrieved 2017-xi-nineteen .
- ^ Rosenberg, Jacob; Bisgaard, Thue; Kehlet, Henrik; Wara, Pål; Asmussen, Torsten; Juul, Poul; Strand, Lasse; Andersen, Finn Heidmann; Bay-Nielsen, Morten (February 2022). "Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults". Danish Medical Bulletin. 58 (2): C4243. ISSN 1603-9629. PMID 21299930.
- ^ "Inguinal hernia". Mayo Clinic. 2022-08-11.
External links [edit]
- Indirect Inguinal Hernia - University of Connecticut Health Center
-
 Media related to Inguinal hernia at Wikimedia Eatables
Media related to Inguinal hernia at Wikimedia Eatables

Source: https://en.wikipedia.org/wiki/Inguinal_hernia
Posted by: johnstoncates1991.blogspot.com
0 Response to "How To Repair Small Left Inguinal Hernia Containing Fat"
Post a Comment